

TL;DR
➡ First viability for hair transplants was seen in a thesis by Dieffenbach in 1822, and in 1897 the first hair transplant was carried out by dermatologist Dr. Menahem Hodara.
➡ The famous Hamilton scale that we use even nowadays for determining a patient’s level of baldness was developed in 1951.
➡ Recent findings show that Dr. Okuda used an older version of FUE in 1939, years before Dr. Orentreich invented the hair plug technique in the 1950s.
➡ With the development of DHI in 1999, an advanced version of the FUE, the golden standard for hair transplants became clear and is still the primary technique.
Believe me, as a doctor doing hair transplants for more than seven years, even I was baffled about hair transplantation history. When you search online, you see different sources explaining different stories. Who invented what in which year; all messed up in sourceless blogs.
I’ve written this article based on the literature to shed light on this mess.
Of course, nobody can know about ancient civilizations trying such a thing since there is no written source. Even recent studies such as a Japanese dermatologist Dr. Shoji Okuda’s during World War II were unrevealed in 2004.
So it is easy to be forgotten by history.
However, we can dig out the documented hair transplantation trials using the literature. According to it, many physicians seem to contribute to the development of modern hair transplantation. I want to thank each of them for helping people become the best version of themselves via hair restoration operation.
This article, in many ways, exists because of them and, thus, is dedicated to them accordingly:
Table of Contents
Myths About the History of Hair Transplantation
Myth 1: Hair transplantation was invented by New York dermatologist Norman Orentreich in 1952.
👉 Dr. Orentreich didn’t conduct the first hair transplant attempts; it began in 1822 with a doctoral thesis of Dieffenbach in Germany.
Even if Dieffenbach didn’t complete a proper hair transplant, he showed the viability of autotransplantation on animals and himself using goose quills as extractors. He completed [1]:
- Bird feather transplantation.
- Auto hair transplantation to his arm.
Myth 2: Hair Plug is an older surgical technique than Follicular Unit Extraction (FUE) Technique.
👉 Dr. Orentreich invented the hair plug technique in the 1950s, and people thought hair plugs were older than FUE.
However, in a paper published in 1939, Dr. Okuda explained the outcomes of successful hair transplantation by using tiny punches to extract follicular units (similar to modern FUE punches) and implanting units in bald sites. He even did an eyebrow transplant [3].
Even if his study was published in the Japanese Journal of Dermatology and Urology, his and his colleagues’ work remained hidden for decades due to the chaotic environment of World War II.
The Chronological Events in Hair Transplant History
👇 Feel free to use the infographic below on your website by linking this page as a source.

1822 – First Feather and Hair Transplant in Wurzburg, Germany by Dieffenbach
As I explained above, the history of hair transplants starts with Dieffenbach’s PhD thesis explaining autotransplantation techniques and clinical trials in the 19th Century.
He conducted successful hair transplant experiments on birds extracting and implanting feathers [1].

1897 – First Hair Transplantation on a Real Patient in Istanbul, Ottoman Empire by Dr. Menahem Hodara (1869 – 1926)
Dr. Hodara was an Ottoman dermatologist born in 1869 in Istanbul, Turkey and is famous for his hair transplant trials [3].
He founded the Society for Dermatology and Venereology of Turkey, of which our dermatologists are members, in 1919 and became the first president.
In his hair transplantation experiments, he cut patients’ hair and trimmed them into various lengths from 1 to 4mm. Then he made incisions on scars left bald by tinea capitis (a.k.a favus or fungal infection), waited until the bleeding stopped, and steeply implanted hairs into incisions.
After a month, he observed that although many of the transplanted hairs were gone, adequate amounts grew to cover a large bald patch caused by the disease. After 3-4 months, some of the hairs left become colored and strong.
In his publication, he stated that although this technique is early, it was a promising starting point and could be further improved with new methods.
After publishing his works, the trial gained massive media attention from the international press. Some newspapers put very assertive titles like “Baldness Conquered” and “No More Bald Heads” [3].
![A cartoon of Dr. Hodara as a barber, Musée des Familles in 1899 (Courtesy of the Bibliothèque Nationale de France, Paris) [2]](https://www.unitedcareclinic.com/wp-content/uploads/2022/01/a-cartoon-of-dr-menahem-hodara-paris-1899-1.jpeg)
1930 – Early Follicular Unit Extraction (FUE) Methods in Japan
The Japanese School of Dermatology has become the pioneer school in developing FUE.
Dr. Sasagawa conducted the first-ever surgical operation for hair restoration in 1931. He placed hairs into bald patches caused by scarring alopecia (a.k.a cicatricial alopecia) using a special needle [3].
Dr. Okuda published five articles called “Okuda Papers” in a row starting in 1939 about hair transplantation. In the article, he clearly explained how skin fragments are removed from the side and back of the hair-bearing scalp using punches and implanted on bald sites on the scalp, eyebrow, and other parts of the body [3].
👉 Okuda was the first doctor to employ self-made sharp punches in 2-4 mm diameters to extract individual hair follicles. He suggested not using 1 mm diameter punches since the rates of harming grafts by transection were relatively high in 1 mm extractions [4].
Unfortunately, World War II caused his works originally written in Japanese pictographs to remain hidden for decades [5]. Dr. Yoshihiro Imagawa discovered and transplanted “Okuda Papers” into English 65 years later in 2004.
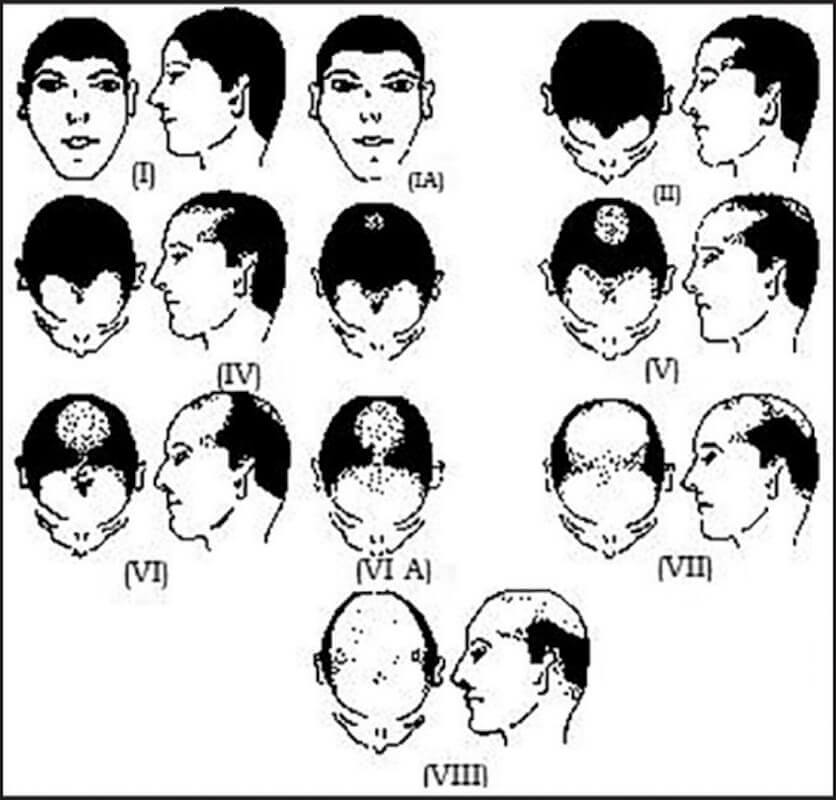
1951 – Hamilton Scale by Dr. James Hamilton
James Bruce Hamilton was an anatomist in New York and an expert on androgenic alopecia.
🔔 He worked on the relationship between male hormones, life expectancy, and baldness and coined the “Male Pattern Baldness” term, known as Androgenetic Alopecia or AGA.
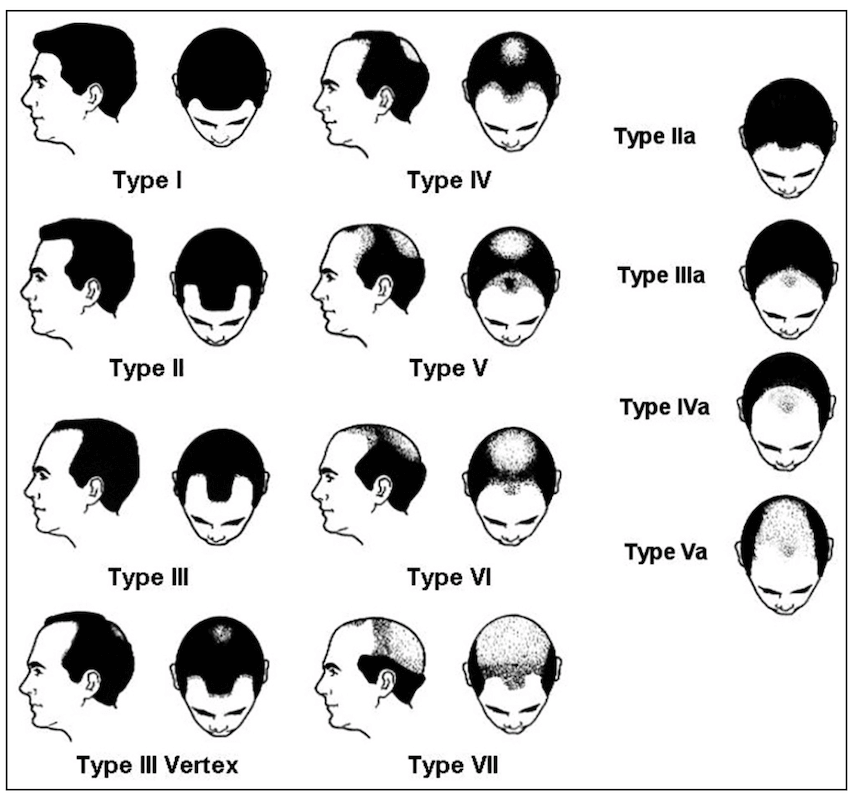
After analyzing more than 300 males with hair loss, he developed a classification system based on balding regions on scalp topography [13].
The Hamilton Classification System consisted of 8 progressive aspects and three subcategories:
- Type I, II, III scalps are not bald
- Type IV – VIII scalps are bald
1952 – Hair Plugs
Unaware of Okuda Papers, New York Dermatologist Dr. Norman Orentreich began hair transplantation experiments using much larger punches than Okuda. He moved a group of follicles consisting of dozens of grafts from the back of a scalp to recipient zones [7].
While experimenting with hair movement, he discovered that grafts taken from the back of the scalp keep their shedding resistance feature in the bald regions. This discovery made him realize that characteristics of hairs in different zones are different; back scalp hairs are more resistant to hair loss [7].
Then he named this characteristic “The Principle of Donor Dominance.” It states that follicles taken from the back and sides of the scalp continue permanently producing healthy hair grafts in recipient zones [7].
The principle initiated the rise of a new billion-dollar hair transplantation industry. Hair transplant surgery has become a standard medical procedure since then.
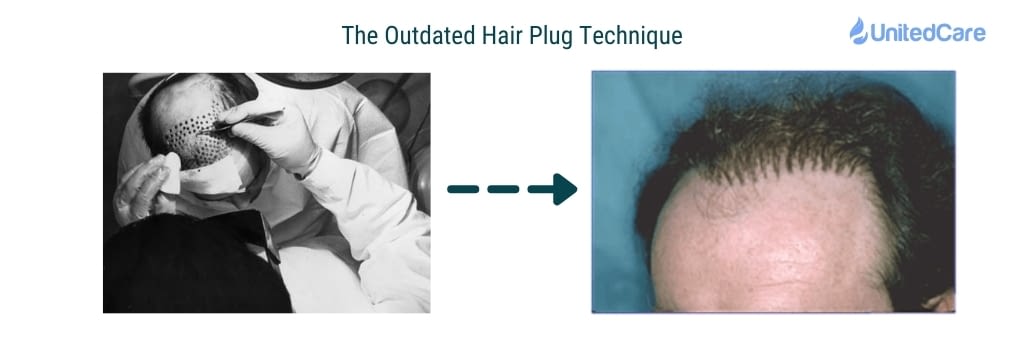
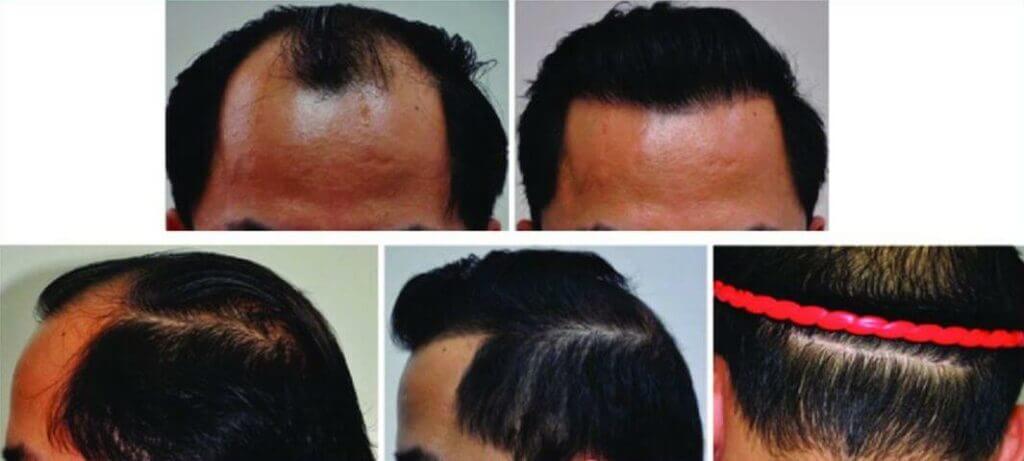
However, the hair plugs technique has a significant downside: Unnatural and unsatisfactory cosmetic results. The result is often called “Doll’s Hair”. Everybody could tell whether a patient has hair restoration surgery.
Below is the result of Dr. Orentreich’s hair plug operation. On the top picture, the right side of the frontal scalp of the patient is shown, and no plugs were implanted in this zone. The left frontal scalp with transplanted hair plugs is shown on the bottom. As you can quickly realize, the look is unnatural and cosmetically unacceptable.
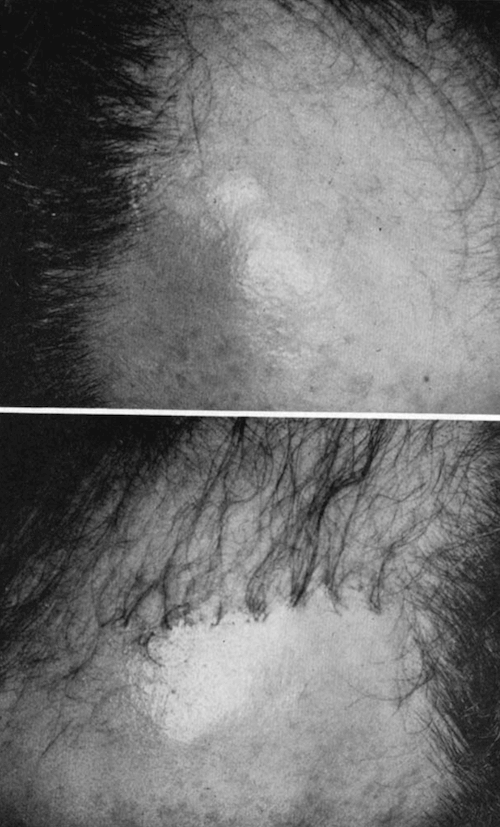
The reason was huge punch tools to harvest groups of donor grafts consisting of 10-20 follicles. These punches were between 6-12 mm in diameter. (Remember, Okuda’s punches were between 2-4mm in diameter).
Another disadvantage of the hair plugs technique was that plugs were so large. It limited the maximum number of plugs transplanted in a session.
For example, deep frontal hairline recessions required 150 hair plugs and four months to complete. Large spots in both frontal and crown areas took 5-6 months to move 500-600 hair plugs [8].
⚠️ In addition, this technique was quite harmful to the donor hairs and health. Big punches were creating big wounds in donor zones, and these wounds were leaving scars after healing.
Even if the development of hair plugs made hair transplantation a medical operation, advancements were needed.
1975 – Hamilton – Norwood Scale by Dr. O’Tar Norwood
After working on patterned hair loss in 1000 men, a dermatologist hair transplant surgeon Dr. O’Tar Norwood updated The Hamilton Classification System in 1975.
Since then, the Hamilton-Norwood Scale has become the hair transplant industry standard and the most widely used classification for Androgenetic Alopecia (Male pattern baldness).
Would you like to find out your hair loss type?
Get a free consultation from our expert dermatologists now:
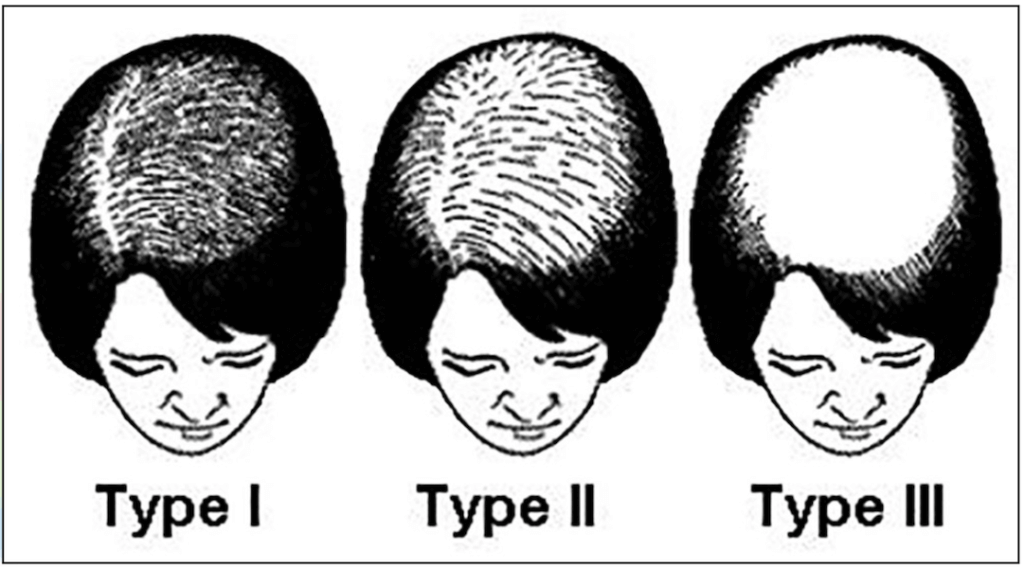
1977 – Ludwig Scale, Classification of Female Pattern Hair Loss
Dr. E. Ludwig analyzed 468 women with hair loss. He created a female pattern hair loss classification system based on the stage of progression [13].
It was the first scale to classify female pattern baldness.
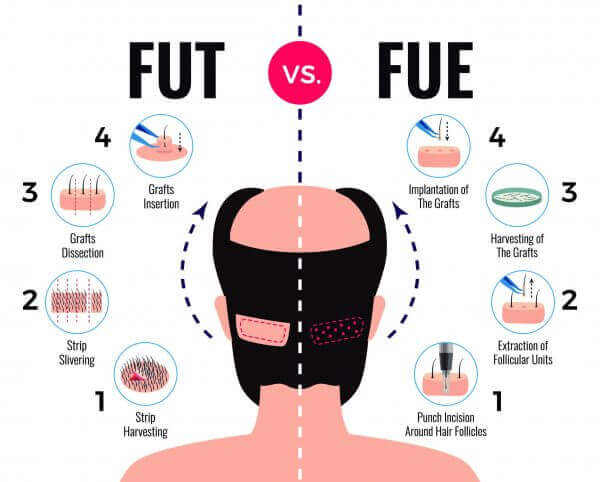
1988 – Follicular Unit Transplant a.k.a. Strip Surgeries
If big punches cause wounds, scars, and unnatural looks, then smaller punches can be used to harvest groups of follicles. It’s a no-brainer.
Employing tinier punches is precisely what doctors started to do. However, even in smaller punch sizes (3-4 mm), “doll head” appeared in the result.
Then, they decided to split the plugs into smaller tissue pieces and tightly implant them in bald zones. The smaller plugs or pieces were called “micro grafts” or “mini grafts”, and the techniques were called “micro grafting” and “mini grafting”.
The hair restoration surgery outcomes instantaneously improved with these new methods. Doctors divided groups into more delicate parts using microscopes and got better results.
However, even if extracted plugs were divided into smaller pieces for better appearance, large punches were still used and spoiled the donor zone look.
Dr. Bobby Limmer came up with the idea of taking out a single strip of skin from the donor area and stitching the open area together to get a better appearance in donor sites. By this method, he could also extract more grafts in a single session [16].
He then dissected donor strips into follicular unit grafts without harming the hair root, hair bulb and hair shaft. Then, these delicate individual follicles were grafted into recipient zones with forceps.
The technique became known as Follicular Unit Transplantation or strip method. In this technique, 2500 or more grafts could be transplanted in a single session, and this amount resulted in excellent coverage of bald spots and high hair density.
With strip harvesting and follicular unit grafting (FUT), modern hair transplant surgeries have become widespread all over the world,
Unfortunately, there was still a problem: the strips were leaving permanent scars on the back of the scalp. FUT hair replacement surgery patients shouldn’t use short hair to hide donor strip scars.
1988 – Follicular Unit Extraction (FUE)
While Dr. Bobby Limmer was developing FUT, a Japanese Dermatologist, Dr. Masumi Inaba was working on a technique similar to modern FUE, with a two-step extraction technique. It is speculated that Dr. Inaba’s contribution to literature played a significant role in developing modern-day FUE [3].
During the same period, Dr. Ray Woods was also doing similar experiments, resulting in his version of FUE named “Wood’s Procedure”. In 1989, he publicly demonstrated Wood’s FUE Procedure [3].
The difference between early FUE and Hair Plugs was the tinier wound size caused by 1mm or smaller punches. Suppose the patient was healthy and following pre-and post-op instructions after an early FUE surgery. In that case, his donor zone was healing rapidly and leaving very little or undetectable-to-eye scar behind. This characteristic of FUE has made it “Gold Standard” in hair transplantations since then.
In 2002, Dr. William Rassman and Dr. Robert Bernstein published “FUE: Minimally Invasive Surgery for Hair Transplant” and coined the term Follicular Unit Extraction [3].
In 2017, ISHRS (The International Society of Hair Restoration Surgery) renamed Follicular Unit Extraction as Follicular Unit Excision. The society stated that excision is a more appropriate and self-explanatory term for the operation. Luckily, the abbreviation remained the same [10].
FUE: Excision = Incision + Extraction
In modern FUE surgeries, it is possible to transplant 4000-4500 grafts in 6-8 hours.
1999 – The Direct Hair Implantation, DHI [6]
DHI is a type of advanced FUE technique developed to fix inherent flaws of FUE/FUT implantations.
Pre-made incisions should be made in classic FUE and FUT before inserting the grafts doubling the work and increasing the error ratio due to the lack of angle and depth control.
Furthermore, In FUT and FUE operations, grafts could be easily damaged in the hands of inexperienced hair restoration surgeons (Keep in mind that some clinics even employ non-medical technicians and nurses to do the surgical procedures which is a clear red flag). The tool that is called forceps is used in the extraction and implantation stages. Its performance heavily relies on the performer.
E.g., if a performer squeezes forceps too hard while pulling or pushing, grafts could be damaged.

To solve these problems, The DHI Medical Group invented DHI Implanter, a handheld device for simultaneous incision and implantation.
The pen allows surgeons to insert grafts without the need for pre-cut incisions. The operator can easily control the implant’s angle, direction, and depth using the implanter pen to make implanted hair look more natural than FUE/FUT.
In addition, it is speculated that the individual graft survival rate and hair growth rates are higher since grafts are directly implanted with minor damage. Also, the longer you keep the grafts outside the body, the lower the survival rate. However, there is no study proving the effectiveness of DHI in terms of survival rates.

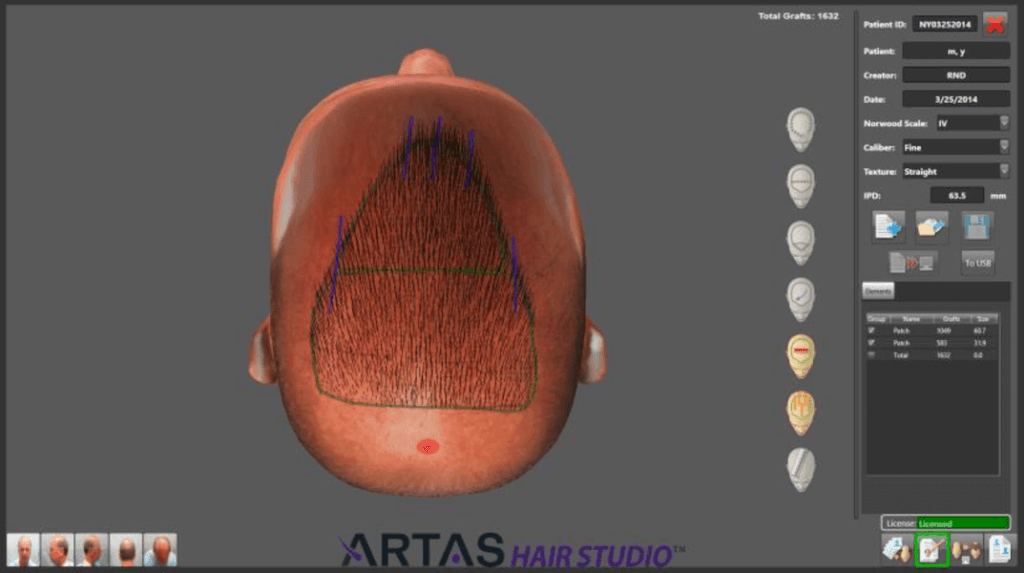
2007 – Robotic Hair Transplant
Humans do not perform the same every time; the performance fluctuates depending on many variables such as fatigue, stress, and emotions.
Modern hair transplant surgeries last 6-10 hours, and the duration depends on the total graft count transplanted. Even if performers start the operation vigorously in the morning, they become tired during the implantation stage at the end of the day. Therefore, the quality of outcome, the ratio of survivorship of grafts may change in this part.
Robots come into play to fix these performance fluctuation-related issues. They are accurate and perform the same if external variables are constant; their output is predictable.
Robots can be configured to automatically do high-precision tasks at breakneck speeds, which increases efficiency and productivity [10].
In 2007, again, Dr. Bernstein and Dr. Rassman, leaders of modern FUE, introduced Robotic Hair Transplant in an ISHRS meeting. By 2011, the ARTAS hair transplantation robot was given FDA approval and entered the marketplace as the first commercially available hair restoration robot [3].
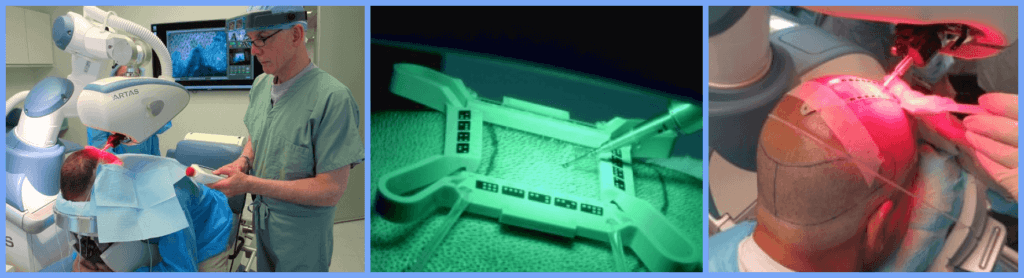
In addition, the dermatologist hair transplant surgeon can focus on more critical and subjective parts of the hair restoration operation; patient eligibility, patient education with pre-and post-op instructions, bald spot coverage, and hairline design.
However, hair transplantation robots are still in development and are not perfect. Some drawbacks are incredibly high cost, lack of judgment, inability to handle extreme cases [11].
Which Hair Transplantation Surgery Technique Should You Choose?
First of all, a patient should make sure he can get a hair transplant operation and his hair loss type definitely requires surgery.
💡 Medical history, ethnicity, hair color, family background, hair thickness, hair thinning and many other variables should be considered in this decision.
An experienced dermatologist hair transplant surgeon specializing in skin, dermal papilla, scalp, and hair could determine patient surgery eligibility after an examination.
The best-suited technique for your hair’s best version is right here.
Our expert dermatosurgeons can help you discover which is the right one:
Keep in mind that if a patient has a skin and scalp disease or exceptional condition, a dermatologist should handle them first. Otherwise, even transplanted scalp hairs may fall pretty soon. A practitioner, nurse, or technician cannot detect such conditions and handle complications of hair transplants resulting in hair transplant rejections or hair transplant failures.
Some cases may not require cosmetic surgery to stop hair loss, restore the lost hair and increase hair density. In this case, hair massage, pharmacological treatments (Minoxidil or Finasteride), PRP, stem cell treatments and diet & lifestyle changes could be the hair loss remedy.
At UnitedCare, we only perform Sapphire FUE and DHI, even if there are other types of hair transplants. We believe that these two types of FUE techniques are the best ones for our patients.
Finally, let me note that in all modern techniques, shock loss occurs in 2 months, and it is a natural process, and the method can’t change it. Healthy hair regrows soon after the shock loss.
Frequently Asked Questions (FAQs)
When was hair transplant invented?
In 1822, the first known autotransplantation was done by Ph.D. student Dieffenbach in Germany. He showed the viability of autotransplantation on animals and himself using goose quills as extractors [1].
Who did the first hair transplant?
In 1897, Dr. Menahem Hodara, an Ottoman dermatologist, did the first hair transplant on an actual patient in Istanbul. After 3-4 months, some of the hairs Dr. Hodara transplanted became colored and strong.
What is the most successful hair transplant procedure?
FUE is the most successful hair transplant procedure since it heals rapidly. In addition, the DHI procedure, a more advanced FUE method, allows its operator to easily control the implant’s angle, direction, and depth using the implanter pen, resulting in a perfectly natural look.

REFERENCES
1. Unger, Walter P. “The history of hair transplantation.” Dermatologic surgery 26.3 (2000): 181-189.
2. Tekiner H, Karamanou M. The forgotten hair transplantation experiment (1897) of Dr. Menahem Hodara (1869 − 1926). Indian J Dermatol Venereol Leprol 2016;82:352-355
3. Bansod S, Kerure A, Rohatgi S, Bilewar U. History of follicular unit excision. Indian J Dermatol Venereol Leprol. 2021 Mar-Apr;87(2):315-318. doi: 10.25259/IJDVL_1071_20. PMID: 33769760.
4. Kayiran O, Cihandide E. Evolution of hair transplantation. Plast Aesthet Res 2018;5:9. http://dx.doi.org/10.20517/2347-9264.2017.86
5. https://en.wikipedia.org/wiki/Hair_transplantation
6. https://www.ishrs-htforum.org/content/19/6/200
7. Orentreich, N. (1959), AUTOGRAFTS IN ALOPECIAS AND OTHER SELECTED DERMATOLOGICAL CONDITIONS. Annals of the New York Academy of Sciences, 83: 463-479.
8. Unger WP. Hair transplantation in male-pattern alopecia. Can Med Assoc J. 1971;105(2):177-181.
9. Rassman, W.R., Bernstein, R.M., McClellan, R., Jones, R., Worton, E. and Uyttendaele, H. (2002), Follicular Unit Extraction: Minimally Invasive Surgery for Hair Transplantation. Dermatologic Surgery, 28: 720-728.
10. https://www.ishrs-htforum.org/content/28/1/1.1
11. Dua A, Dua K. Follicular unit extraction hair transplant. J Cutan Aesthet Surg. 2010;3(2):76-81. doi:10.4103/0974-2077.69015
12. https://www.bernsteinmedical.com/robotic-hair-transplant/
13.Gupta, Mrinal & Mysore, Venkataram. (2016). Classifications of Patterned Hair Loss: A Review. Journal of Cutaneous and Aesthetic Surgery. 9. 3. 10.4103/0974-2077.178536.
14. https://www.ishrs-htforum.org/content/25/5/177.full
15. https://dhiglobal.com/about/milestones/
16. Limmer BL. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. J Dermatol Surg Oncol. 1994 Dec;20(12):789-93. doi: 10.1111/j.1524-4725.1994.tb03706.x. PMID: 7798409.